Behavioral documentation is one of the most important parts of memory care. Healthcare can offer residents complete service by observing their moods, behaviours, daily activities and responses to various stimuli. This is especially important for residents with dementia. The behaviours exhibited by these residents usually reflect their emotions and thoughts, but because they cannot speak, we are unable to ask them directly for their opinions.
Documentation allows us to provide residents with the most secure, appropriate and tailored approach to care, but when documentation is done poorly (incorrectly), quickly (rushed), or incompletely, we may be putting the residents in jeopardy if we miss warning signs or symptoms. This means that they may experience higher levels of stress, pain and discomfort than necessary, and potentially suffer from additional negative (health) outcomes.
Here in this blog, we are going to explain why accurate behavioral documentation matters. We will also discuss the common challenges staff face and how AI documentation tools are helping improve the process. It also shares best practices for care teams and looks at the future of documentation in memory care.
Understanding Behavioral Documentation in Memory Care
Behavioral documentation is a daily part of caregiving in memory care communities. Staff members track information about residents’ actions, moods, reactions, routines, and changes. These notes help care teams understand what residents need and how to support them better.
Why Behavioral Documentation Matters
Behavioral documentation gives meaning to what might otherwise look like random or unpredictable actions. When staff record behaviors consistently and clearly, patterns begin to appear. These patterns help care teams understand what triggers certain behaviors and how to respond in supportive ways.
Documents play a critical role in helping employees track changes to care plans; by tracking potential disruptors (appetite, sleep pattern, etc.), they’re then able to notice when those changes occur, which ultimately leads to quicker identification of an infection/discomfort/emotional distress.
Without written records of minor changes in a resident’s daily life, there is a risk that any changes will go unnoticed, resulting in residents not receiving adequate care. The written record serves as a critical tool in keeping both the employee and the resident informed of their needs and encourages employees to act promptly.
Understanding Behavioral Patterns in Dementia
People with dementia often show behaviors linked to memory loss, confusion, or changes in their environment. These behaviors may include:
- Agitation
- Wandering
- Repetitive speech or actions
- Withdrawal
- Resistance to care
- Sudden mood changes
Through systematic documentation of individual behaviour patterns, caregivers are able to identify some of the potential causal events. A resident might become agitated during bathing, when exposed to loud noises, or whenever the resident’s routine(s) have been disrupted. Based on accurate documentation of these events, the care provider(s) can adjust the environment (i.e., reduce noise) and/or approach the resident differently and increase the level of comfort for the resident.
Identifying Early Health or Mood Changes
Behavior is often the first sign that something is wrong. Residents with dementia may not be able to explain pain, discomfort, or anxiety. Instead, they may show changes in:
- Sleep pattern
- Appetite
- Level of engagement
- Physical movement
- Verbal expression
Accurate documentation in memory care helps staff notice these small changes early. Early detection means care teams can intervene quickly. This improves resident safety and reduces the chance of hospital visits or emergencies.
Challenges in Behavioral Documentation in Memory Care Teams
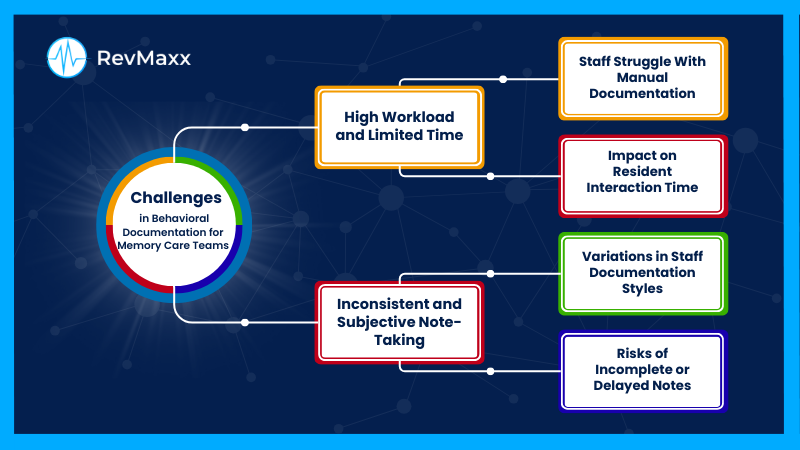
Despite its importance, behavioral documentation is not always easy. Staff are busy, often balancing many tasks at once. Memory care settings also have ongoing activities and unpredictable situations that make documentation challenging.
High Workload and Limited Time:
Care teams in Memory Care work in fast-paced environments. They help residents with daily routines, activities, personal care, medication reminders, and emotional support. Documentation often happens in between tasks or at the end of the shifts.
Why Staff Struggle with Manual Documentation
Manual documentation in memory care takes time. Staff must stop what they are doing, write down their observations, and make sure the notes are accurate. When the workload is heavy; documentation may be rushed or postponed. This leads to missed details or incomplete notes.
Paper documentation is especially difficult because it requires staff to carry forms, find space to write, and later transfer the information into digital records. This increases chances of errors, delays, and inconsistencies.
Impact on Resident Interaction Time
Every minute spent writing notes is a minute less spent with residents. Memory care teams often want to spend more time:
- Talking with residents
- Supporting activities
- Building trust
- Responding to emotional needs
But documentation pressures can reduce this valuable interaction time. When staff feel rushed, they may write shorter notes or skip small details that are actually important for care planning.
Inconsistent and Subjective Note-Taking:
Another challenge is inconsistency among different caregivers. Every person has their own way of describing behaviors, moods, or reactions. This makes documentation subjective.
Variations in Staff Documentation Styles
Some staff members write long descriptions. Others write short, simple notes. Some focus on behavior, while others focus on the situation. Because there is no single style, the documentation varies greatly. This inconsistency can make it difficult to understand patterns or compare notes across shifts.
For example, two caregivers may describe the same behavior differently:
- “Resident was agitated.”
- “Resident yelled during lunch and tried to leave the dining room.”
The second note gives clearer information. But without standard guidelines, documentation styles remain inconsistent.
Risks of Incomplete or Delayed Notes
When notes are incomplete or written long after the behavior occurs, important details are lost. Staff may forget:
- What triggered the behavior
- How long it lasted
- Who was present
- What helped calm the resident
- Whether the behavior was unusual
Delayed documentation in memory care also makes it hard for the next shift to understand what happened. This limits continuity of care and increases the chance of repeated issues.
How Accurate Behavioral Documentation Improves Resident Outcomes
Accurate documentation benefits residents, families, and care teams. It strengthens communication, improves safety, and supports better care planning.
Supports Personalized Care Planning
Every resident is unique. They have different histories, health needs, routines, preferences, and triggers. Accurate behavioral documentation helps care teams design care plans that truly reflect the resident’s needs.
Tailoring Activities and Routines
When staff track reactions to activities, meals, or daily routines, they can identify what works best for each resident. This helps in:
- Creating calming routines
- Reducing stress or confusion
- Improving participation in activities
- Offering support at the right time of day
A resident may feel calmer in the morning, enjoy music therapy, or respond well to familiar objects. Documentation helps care teams build these insights into daily schedules.
Improving Safety and Reducing Incidents
Many safety issues in memory care come from unrecognized behavioral changes. Wandering, resistance to care, falls, or agitation often have triggers. With accurate documentation, staff can identify these triggers and adjust the environment.
For example:
- If a resident becomes restless around 4 pm (sundowning), staff can plan calming activities.
- If a resident wanders after meals, staff can increase supervision during that time.
- If a resident shows signs of discomfort before bathing, staff can adjust the approach or timing.
Better documentation leads to fewer incidents and a safer environment.
Strengthens Communication Across Care Teams and Families
Clear documentation helps all members of the care team stay updated. It also supports transparent communication with families, which is essential for trust and peace of mind.
Consistent Updates for Interdisciplinary Teams
Behavioral notes are not only useful for caregivers. Nurses, therapists, physicians, and administrators all rely on this information. Accurate documentation in memory care supports teamwork by ensuring that everyone sees the same information, understands trends, and contributes to better decision-making.
Transparency for Families and Caregivers
Families want to stay informed about their loved one’s health and well-being. Accurate documentation helps staff share updates during family meetings or care plan reviews. When families understand the resident’s behavior patterns and how staff respond, they feel reassured and more involved.
The Role of Technology in Enhancing Behavioral Documentation
Technology is transforming how care teams document behaviors. Digital tools make the process faster, more accurate, and easier to manage.
Real-Time Recording and Tracking
Digital tools allow staff to record behaviors as soon as they observe them. This reduces the risk of forgetting details and improves overall accuracy.
Documenting Behaviors Immediately at the Point of Care
With mobile devices, tablets, or handheld tools, staff can document behavior while they are with the resident. This helps capture:
- Exact time and place
- Triggering events
- Actions taken
- Resident response
Real-time documentation supports better decisions, especially during shift changes.
Reducing Memory-Based Errors
When staff rely on memory, they may forget details or mix up situations. Technology reduces this risk by allowing immediate entry. This results in clearer, more reliable notes.
Digital Tools Supporting Accuracy
Digital platforms help standardize documentation across teams. They offer templates, forms, and structured fields that ensure consistent reporting.
Standardized Templates and Forms
Templates guide staff on what information to record, such as:
- Type of behavior
- Intensity
- Duration
- Environmental triggers
- Staff interventions
Consistent formats reduce subjective language and ensure that important details are always captured.
Easier Access to Resident History
Digital systems store all notes in one place. Staff can quickly look up past behaviors, compare changes over time, and understand patterns. This historical information is essential for care planning and safety.
How AI Tools Like RevMaxx Transform Behavioral Documentation
AI-powered tools are making documentation faster, easier, and more accurate for memory care teams. By reducing manual work, staff gain more time for direct resident support.
Automated Note Creation for Behavior Tracking
One of the biggest advantages of RevMaxx is automated note creation. The tool listens to what staff observe and turns it into clear, structured notes. This means caregivers no longer have to remember every detail during busy shifts. They simply report what they see, and the system organizes it in the right format.
Automation also helps remove guesswork. Notes become more objective and less dependent on individual writing styles. This supports better communication across teams and keeps everyone on the same page.
Voice-to-Text Capture for Faster Notes
With voice-to-text, staff can document while standing beside the resident. They do not need to step away, find a computer, or flip through paper forms. They just speak naturally, and the system converts the information into clean, readable notes.
This feature is extremely helpful during:
- Evening rounds
- High-activity periods
- Behavior escalations
- Medical emergencies
- Times when staff must stay close to residents
Voice-to-text ensures that important details are not forgotten. It captures information immediately, even when the day gets hectic.
Reducing Manual Workload and Fatigue
Manual documentation in memory care, where behaviors change frequently. Staff often fill out multiple forms, write long descriptions, and repeat information between systems. This leads to physical strain, mental fatigue, and time away from residents.
RevMaxx reduces this workload. Instead of writing everything by hand, staff only need to speak or tap through guided prompts. This keeps documentation accurate without adding stress. Caregivers feel lighter, more focused, and more able to support residents with calm, patient attention.
Less paperwork also means fewer errors, fewer delays, and more energy for hands-on care.
Seamless Integration With EHR Systems
Another major benefit of RevMaxx is, how smoothly RevMaxx integrates with popular electronic health record (EHR) systems like Epic, eCW, PointClickCare, Pratice Fusion, NextGen etc. There is no need to switch between platforms or re-enter the same details. Everything flows automatically into the resident’s main chart.
This reduces confusion and keeps information in one place. Nurses, therapists, and physicians can easily review notes and understand the resident’s current state.
Syncing Behavioral Notes With Care Plans
When behavioral documentation in memory care syncs directly with care plans, updates happen in real time. If a resident shows new patterns, such as increased restlessness, changes in appetite, or frequent wandering, the care plan adjusts quickly.
This helps the wider team make better decisions. They can modify routines, add interventions, or collaborate on new safety measures. Nothing gets overlooked because everyone is working with the same updated data.
Real-time syncing also supports smooth shift-to-shift communication. Incoming staff understand exactly what happened earlier and what needs attention next.
Ensuring Compliance and Data Consistency
Accurate documentation is not only helpful—it is required. Memory care communities must follow strict guidelines for reporting behaviors, incidents, and care interventions. Missing notes or inconsistent entries can create compliance risks.
RevMaxx helps avoid these issues by keeping documentation:
- Structured
- Complete
- Time-stamped
- Stored in the correct place
- Easy to retrieve during audits
Standardized templates reduce variation between caregivers. Automated reminders help ensure that nothing important is skipped. This creates a clean, consistent record for every resident.
Best Practices for Effective Behavioral Documentation in Memory Care
Behavioral documentation is most effective when care teams follow simple but important best practices.
Using Clear, Objective, and Descriptive Language
Staff should avoid vague words like “agitated” or “upset.” Instead, they should describe what they saw:
- “Resident yelled loudly for five minutes.”
- “Resident walked out of dining room and tried to exit the hallway.”
Clear descriptions help other team members understand what actually happened.
Charting in Real Time
The closer the documentation is to the behavior, the more accurate it will be. Staff should try to document:
- Immediately after the event
- During routine rounds
- Before shift handover
Real-time documentation supports safety and continuity.
Leveraging Mobile or AI Tools for Accuracy
Mobile devices, digital forms, and AI-powered tools make documentation easier and more reliable. Staff get guided prompts, voice capture, and reminders to ensure no details are missed.
The Future of Behavioral Documentation in Memory Care
The future of memory care will rely on more advanced, intuitive, and intelligent documentation tools. As technology evolves, behavioral notes will become more precise, more consistent, and more accessible.
Future trends may include:
- Automated behavior recognition
- Predictive tools that identify early risks
- More personalized care plans built on long-term behavior patterns
- Stronger communication between families and care teams
- Reduced paperwork and increased caregiving time
With better documentation in memory care communities will offer safer, calmer, and more supportive environments. Residents will benefit from earlier intervention, personalized routines, and better overall care.