Many Healthcare Professionals find themselves struggling with their Medical Records Documentation processes – charting, coding, and electronic health record (EHR) entry can be burdensome. The introduction of RevMaxx as an AI Medical Scribe has helped clinicians by enabling them to provide patient care while simultaneously having structured notes written by an AI program as well as the ability to focus on patient care without being distracted by recordkeeping requirements.
RevMaxx has another important feature that makes it advantageous to clinicians, customized specialty templates, it has custom built specialty templates that will accommodate each clinician’s particular specialty/industry, workflow, and individual writing style. This unique custom template feature allows the AI Scribe to provide information that is specific to each clinician’s specialty/industry and to allow clinicians to write more effectively and efficiently than ever before.
So, in this blog, we dive deep into the specialty templates offered by RevMaxx- what they are, why they matter, and how they benefit various types of practices.
Why Customized Specialty Templates Matter
Before jumping into the specifics, it helps to understand why custom templates are so important.
- Different documentation needs: Each medical specialty captures different kinds of data. The layout of a cardiologist’s note is totally different to that of a psychiatrist. RevMaxx understands this and has created specialized SOAP notes based on specialty.
- Time savings for the clinician: Because the template is customized for your specialty, you will spend significantly less time editing because it will be structured in the way you think and work.
- Increased Consistency: Having everyone on your team use the same specialty-specific template will result in a more uniform format for notes, which makes it easier to read, audit and distribute.
- Increased Accuracy of Coding: RevMaxx utilizes these templates to provide excellent ICD-10, CPT, HCC, and E/M codes. Therefore, the structure of your SOAP Notes will help RevMaxx identify billing items much easier.
- Improved EHR-Integration: RevMaxx can quickly push the structured notes directly into your EHR using either RPA or API. Often, the template sections will be mapped to the correct fields eliminating the need for manual copy and pasting.
Key Specialties Covered by RevMaxx Templates
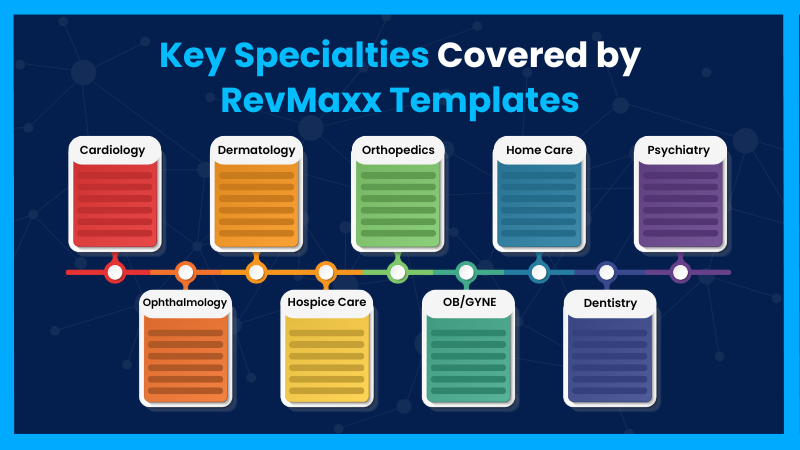
Here are some of the main specialty templates they support—and how they help in each context. RevMaxx doesn’t publicly list every specialty. Here are major specialties and a breakdown of what RevMaxx offers for each:
- Cardiology Template
- Dermatology Template
- Oncology Template
- Primary Care Template
- Hospice Template
- Ophthalmology Template
- Family Medicine Template
- Emergency Room Template
- Psychiatric Template
- Psychology Template
- Osteopathic Medicine Template
Let’s explore each.
Cardiology Template:
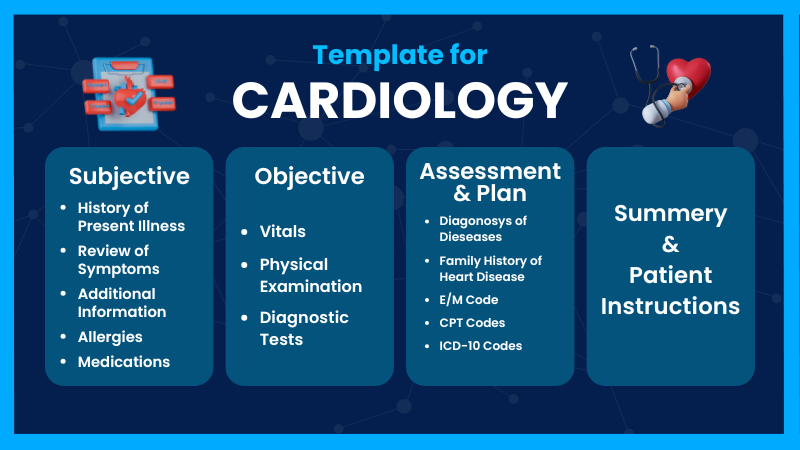
- Subjective: Here patient’s own words are documented: their chief complaint (“chest pain on exertion,” for instance), followed by a structured History of Present Illness (HPI) using cardiac-specific frameworks (onset, quality, radiation, timing, associated symptoms, risk factors like hypertension or family history).
- Objective: In this section, all measurable and observable data are recorded. This includes vital signs (blood pressure, heart rate, oxygen saturation), findings from a physical cardiac exam (such as murmurs, jugular venous pressure, or edema), and any diagnostic test results reviewed during the visit — for example, ECG interpretations, echocardiogram findings, or lab results (lipids, BNP).
- Assessment: Here clinical reasoning is distilled: the cardiologist’s working diagnoses (such as “stable angina” or “hypertension”), differential considerations, and risk stratification are laid out. This part often includes coding-relevant information, allowing RevMaxx to suggest appropriate ICD-10 diagnoses in real time.
- Plan: The next steps: what investigations should be ordered (like stress tests or labs), medication adjustments, lifestyle advice, and any referrals (such as cardiology for catheterization or cardiac rehab). This part also includes patient education — discussing risk, warning signs, and strategies for prevention — and a clear follow-up plan.
- Summary: It can wrap up the note. Here, the cardiologist’s judgment is stated succinctly, summarizing the key diagnosis, rationale, and plan in a few lines.
Dermatology Template
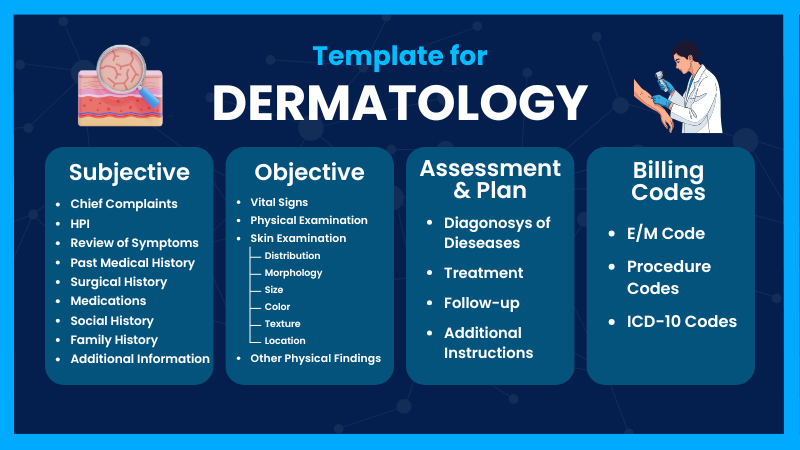
- Subjective: In this section, the provider uses the patient's exact wording to document the patient's concerns. Also included in this documentation is a complete history of the current illness, such as beginning (onset), length (duration), and changes (progression). Additionally, the section should also document any factors that may have contributed to the development of the current condition (trigger), previous treatments used, sun exposure, and other symptoms associated with the condition, such as itchy, painful, etc., as well as additional information, including but not limited to previous and/or current skin problems (e.g. eczema, acne, etc.) and current medications and allergies the patient has.
- Objective: This section documents what the clinician sees on exam. In dermatology, this section must be detailed. This section will describe the lesion’s (size, shape, colour, texture), vital signs if applicable, and procedures performed and give an explanation of the procedure's site, method and reason(s) for performing it.
- Assessment: The most likely diagnosis of the clinician and possible differential diagnoses will be documented in the assessment. It is important to have a brief explanation of the reasoning behind these diagnoses, based on the patient's history and physical examination.
- Plan: The clinician needs to document the treatment(s) they will be prescribing (e.g., topical steroids, antifungals, moisturisers, systemic medications), and include any preventative measures (e.g., sun protection, skin care routine, avoiding triggers). If there is a need for any investigations (e.g., biopsy, patch testing, blood test), they should also be included in the plan.
Oncology Template
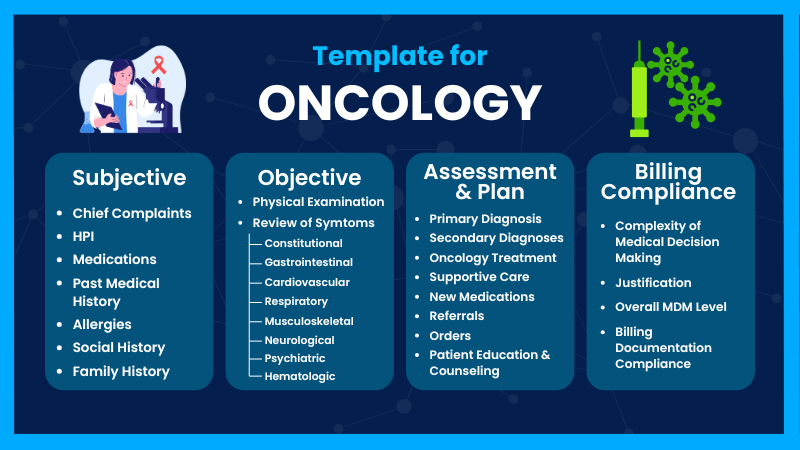
- Subjective: The patient states that "I'm feeling more tired than ever, and I have pain and discomfort in the same place as when I had treatment for my cancer," and thus have a primary concern. To document this concern fully, we would then take a detailed history of the patient's present illness, including the onset, progression over time, what makes the symptoms better, what makes them worse, whether they have any additional symptoms associated such as weight loss, fevers, pain, etc., and finally, whether any other new problems developed since the previous appointment. It should also document the patient’s cancer history (diagnosis, stage, prior therapies—surgery, chemotherapy, radiation), comorbidities, current treatments (including cycles, dose, oral or IV), side-effects, other medications, and allergies.
- Objective: Essential components of this section comprise Body temperature/cardiac rate/body weight/blood pressure/ Heart beat velocity/Respiratory Rate, Clinical evaluations, Diagnostic Indicators(Ex: Tumor Marker, Hemogram, Liver Kidney Assessment), Radiology diagnostics (CT, PET, MRI)/ Recent pathology tests should be provided as overview based on the summary above. The Physical Procedure portion of this investigation includes a detailed account of any Invasive procedures(Ex: Biopsy, Chemotherapy, Central Venous Catheteration, etc.) performed, their location, their method of administration, and the Patient’s response or outcomes.
- Assessment: This section is where the oncologist describes the current working diagnosis or clinical impressions of the patient. The oncologist should also include the differential diagnosis that is being considered such as therapy toxicity vs disease recurrence vs unrelated illness, and should include comments on applicable risk factors and prognostic indicators (e.g. infection risk, organ toxicities). Lastly, the oncologist may use response criteria and performance status (re: RECIST in solid tumors and ECOG/Karnofsky scale) to provide additional context for the patient's disease status.
- Plan: This section provides guidance on what to consider next in the patient's management: changes in therapy, supportive care, research and referrals (palliative care, radiation oncology, clinical studies) and patient education to help them understand potential side effects (e.g., neutropenic fever and bleeding), how to care for themselves, and the need to follow up with their physician when necessary (i.e., when the patient should return; what labs or scans to have done; and when to contact the physician if they experience urgent symptoms).
Primary Care Template
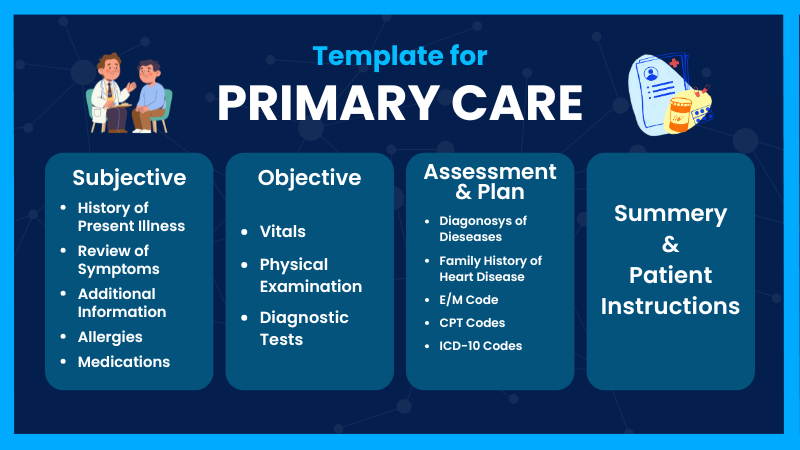
- Subjective: The first major narrative section is Subjective, where what the patient reports in their own words is documented. RevMaxx listens in real time to pick up the chief complaint and then constructs a detailed History of Present Illness (HPI). The template also captures the patient’s past medical history (diabetes, hypertension, chronic kidney disease, etc.), medications (both prescription and over-the-counter), allergies, and a review of systems (ROS) tailored for primary care.
- Objective:Here, the template records all measurable and observed data. RevMaxx automatically transcribes vital signs (blood pressure, pulse, temperature, respiratory rate), physical exam findings (heart, lungs, abdomen, extremities), and any diagnostic data discussed in the visit.
- Assessment: This portion of the medical record summarizes the physician's clinical judgment. The RevMaxx will assist in creating a comprehensive list of the provider's diagnoses and may provide suggested ICD-10 codes automatically.
-
Plan: Primary Care Plans may consist of:
(1) Ordering Investigations,
(2) Prescribing or Changing Medication,
(3) Lifestyle Education,
(4) Preventive Care, and
(5) Follow-up Instructions.
It is also capturing patient education, like provider-patient discussions on self-care and follow-up, including warning signs and decisions shared between provider and patient.
Hospice Template
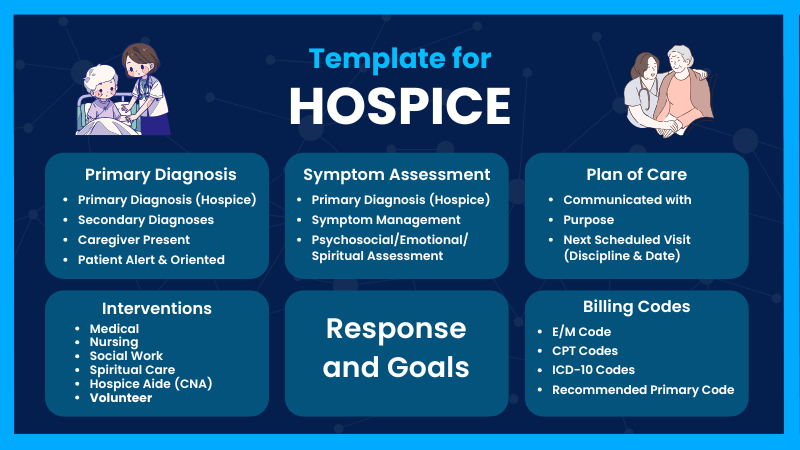
- Patient Identification and Encounter Details: Begin by stating who the patient is, where the encounter is happening, and why. Include basic demographics (age, gender), setting (home, inpatient hospice), and purpose (follow-up, initial evaluation, symptom crisis).
- Prognosis / Terminal Status and Goals of Care: In hospice, it’s crucial to affirm the terminal nature of illness and restate or review the goals of care.
- Symptom Assessment: Here, document comprehensive symptom evaluation. Use standardized symptom scales (for example, ESAS — Edmonton Symptom Assessment Scale) or narrative description. Include emotional / psychological symptoms too: “He feels somewhat anxious about dying, expressing worry about burdening his daughter, who is his primary caregiver.”
- Physical / Functional Status: Discuss physical functioning (mobility, ADLs) and changes since last visit.
- Psychosocial, Spiritual, and Family Context: Hospice care is holistic, so note the social and emotional context, family dynamics, and spiritual or cultural needs.
- Advance Directives, Legal / Compliance: Document the presence (or absence) of advance care planning.
- Plan of Care (Medical and Comfort Measures): Lay out the plan for symptom management and comfort.
- Communication and Family Support Plan: Describe how you will communicate with family and coordinate care.
- Follow-up and Monitoring: Indicate next steps and when you will reassess.
Ophthalmology Template
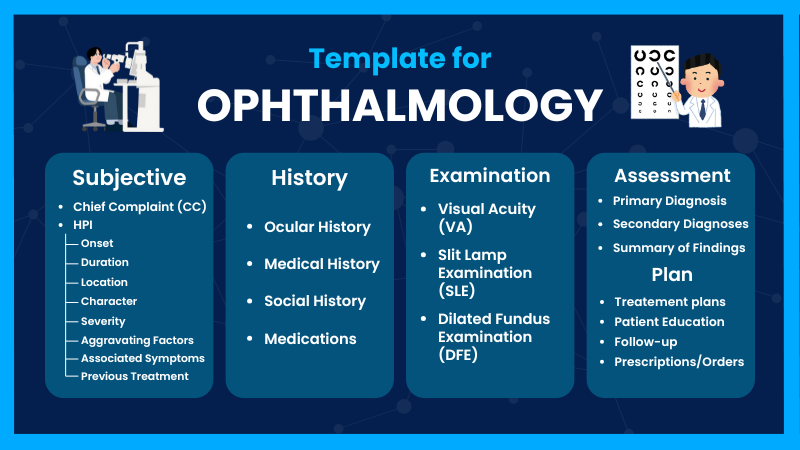
- Patient & Encounter Details: To anchor the note — who, when, and why.
- Chief Complaint & HPI: Describes the vision-related symptoms, their onset, progression, and associated features. Very important in eye care because symptoms like blurriness, floaters, flashes, or pain give diagnostic clues.
- Ocular & Systemic History: Includes past eye conditions (glaucoma, cataract, surgeries), systemic diseases (diabetes, hypertension) that can impact eye health, and family history (glaucoma, macular degeneration). These provide context.
- Medications & Allergiess: Eye drops and systemic meds both matter in ophthalmology. For example, glaucoma drops, steroids, or anticoagulants are relevant.
- Review of Systems (Ocular): Helps capture associated symptoms (pain, flashes, diplopia) that guide differential diagnosis. Many template-guides include a focused ROS.
- Objective Exam, Clinical Findings: This is the core: visual acuity, IOP, slit-lamp findings, pupil reactions, motility, fundus exam. These form your objective data.
- Diagnostic Tests / Imaging: OCT, visual fields, fundus photos, etc. These are crucial in ophthalmology, especially for retina-glaucoma follow-up.
- Assessment / Diagnosis: List your eye diagnoses, with laterality, severity, and differential diagnoses if needed. Templates often map to ICD-10.
- Plan & Management: What you will do — medical therapy, surgery, monitoring, referrals, patient education. It is very important to document follow-up and plan.
- Communication / Coordination: Because ophthalmology often overlaps with primary care, other specialists, or surgical teams, note how you’re coordinating care.
- Summary: A concise wrap-up helps other clinicians quickly understand key problems and plan.
Family Medicine Template:
- Subjective: RevMaxx listens to the conversation and captures the chief complaint in the patient’s own words. It then builds a History of Present Illness (HPI) that is tailored to primary care: onset of symptoms, severity, duration, variation over time, aggravating or easing factors, how this is affecting day-to-day life, and any associated symptoms like cough, fatigue, urinary changes, or GLP-1 medications for weight loss.
- Past Medical History: In family practice, the past medical history is often broad, so the template will include chronic conditions, previous surgeries, hospitalizations, immunization status, family history, and social history. Medications (both prescription and over-the-counter), allergies, and a review of systems (ROS) are also recorded.
- Objective: RevMaxx will transcribe vital signs (blood pressure, heart rate, temperature, respiratory rate, weight), along with findings from the physical exam: cardiovascular, respiratory, abdominal, musculoskeletal, neurological, skin, etc., depending on what was examined. If labs or test results are reviewed during the visit, those are included.
- Assessment: Family medicine providers often manage multiple diagnoses in one visit. For example: “Type 2 diabetes, poorly controlled,” “essential hypertension,” “acute viral pharyngitis,” or “hyperlipidemia.” RevMaxx’s AI can suggest relevant ICD-10 codes based on these assessments.
- Plan: It includes investigations, medication changes, lifestyle advice, and preventive care. It also captures patient education- what the doctor tells the patient about self-care, danger signs, and shared decision-making. Finally, the plan includes a follow-up schedule: when to return, what to monitor, and how to track progress.
Emergency Room Template
- Subjective: It records the patient’s presenting complaint in their own words.The AI scribe picks up key details of the History of Present Illness (HPI): onset, provocation or aggravating/relieving factors, quality, radiation, severity, timing , and associated symptoms. It also captures relevant past medical history, medications, allergies, and a focused review of systems (ROS).
- Objective: This section is available with vital signs, physical exam findings , and any diagnostics performed or reviewed during the visit.
- Assessment: It distills the clinician’s working diagnoses. Because RevMaxx supports coding, the AI suggests ICD-10 codes based on these assessments. The assessment also reflects the clinical reasoning: why, what else is being considered, and risk stratification.
- Plan: RevMaxx structures what to do next in the ER: ordering or repeating labs, initiating treatments, monitoring, imaging, and specialty consults. The plan also includes disposition decisions: whether to admit to a monitored bed, observe, or discharge with instructions. If discharged, the template captures discharge instructions: medications, warning signs, follow-up, and patient education.
Psychiatric Template & Psychology Templates
Psychiatric Template
Psychology Templates
- Subjective: This AI-powered scribe listens to the patient’s account of what brought them in: their chief complaint and builds a detailed History of Present Illness (HPI). In the psychiatric setting, the HPI often covers when symptoms began, their course, provocation or alleviating factors, and associated thoughts or behaviors. The template also records past psychiatric history, previous treatments, current medications, substance use, allergies, and a review of systems (ROS) tailored to mental health.
- Objective: This covers observable and measurable data. Here, RevMaxx will transcribe vital signs, mental status exam (MSE) findings, observable behavior, and other physical or neurological observations. The mental status exam might include appearance, behavior, speech, mood and affect, thought process, thought content , cognition, insight, and judgment. If lab tests, toxicology results, or other investigations are reviewed, RevMaxx captures those too.
- Assessment: The clinician’s diagnostic impressions are recorded in this section. RevMaxx suggests appropriate ICD-10 codes based on these assessments. The assessment also reflects clinical reasoning—why the provider believes a certain diagnosis, what differential diagnoses are being considered, and risk evaluation.
- Plan: This section outlines the next steps: medication management, psychotherapy, safety planning, labs to monitor, and follow-up schedule. It also includes patient education — what the psychiatrist discussed with the patient about treatment options, side effects, expectations, and shared decision-making.
- Subjective: This section follows, where the AI scribe listens to the client’s narrative — what they report in their own words. The history of present illness (HPI) captures more detail: onset, course, what helps or makes things worse, and associated cognitive or emotional symptoms. It also records relevant psychosocial history such as major life events, relationship stress, trauma, work or school functioning, social support, and coping mechanisms. The template includes current medications, any psychiatric or therapy history, substance use, and any allergies.
- Objective: This includes the client’s appearance, behavior, speech, mood and affect, thought processes, thought content, cognition, insight and judgment, and risk factors. If relevant, the note also captures results of any psychological testing or screening tools (e.g., PHQ-9, GAD-7, MOCA), lab tests, or other assessments reviewed in the session.
- Assessment: In this portion, the psychologist’s or mental health clinician’s clinical impressions are summarized. RevMaxx’s AI would suggest appropriate ICD-10 (or DSM-aligned) diagnostic codes. The assessment also includes a reflection on severity, risk (for self-harm, suicidality), and differential diagnoses. The clinician may note treatment response if this is a follow-up.
- Plan: This outlines the therapeutic and clinical strategy. It may also include safety planning if risk is present. Additional orders might include referrals, laboratory work, or screening tasks. The plan also captures patient education and shared decision-making: what was discussed with the patient about therapy goals, the expected timeline for improvement, potential side effects, and follow-up.
Osteopathic Medicine Template
-
Subjective: This is where you capture the patient's history, complaints, and symptoms — largely in their own words, supplemented by the physician’s clarifying questions.
Sections to include:
- Chief Complaint (CC): What brings the patient in today.
- History of Present Illness (HPI): Use OPQRST (Onset, Provoking/Palliating, Quality, Radiation, Severity, Timing) plus any context.
- Past Medical History (PMH): Include relevant medical, surgical, and osteopathic history.
- Medications / Allergies: Current medications, supplements, allergies.
- Social History: Lifestyle factors, occupation, exercise, stress, sleep.
- Review of Systems (ROS): A structured checklist (or narrative) covering relevant systems (e.g., musculoskeletal, neurologic, GI, etc.). The American Academy of Osteopathy recommends a 12-point ROS.
- Patient Goals: What the patient hopes to achieve with treatment (e.g., pain relief, better mobility, avoid medications). -
Objective: This is the clinician’s physical exam, including vital signs, general observation, and detailed osteopathic structural exam.
Sections to include:
- Vital Signs & General Exam: BP, pulse, respiration, general appearance.
- Musculoskeletal / Structural Exam:
1. Document findings of somatic dysfunction using the TART framework — Tissue Texture Abnormalities, Asymmetry, Restriction of Motion, Tenderness. This is standard in osteopathic SOAP note forms.
2. For each region (head, cervical, thoracic, lumbar, pelvis, ribs, extremities), note whether there is TART, and the severity. The osteopathic SOAP forms often use a severity scale (e.g., 0 = none, 1 = mild, 2 = moderate, 3 = severe).
3. Record the specific somatic dysfunction diagnosis: e.g., “C4–5 NRrSl” (meaning restricted motion, etc.), or “left sacroiliac joint shear.”
- Neurological / Other Systems (if relevant): Reflexes, motor/sensory exam, any special tests.
- Pre-OMT Functional Findings: Range of motion (ROM), muscle tone, gait, posture. -
Assessment: This is the clinician’s synthesis: diagnosing, interpreting the exam, and conceptualizing the patient’s problems, including somatic dysfunction.
Sections to include:
- Diagnosis / Impression:
1. List somatic dysfunctions by region. E.g., “Somatic dysfunction: lumbar spine (L4–L5 bilateral NRrSl), pelvis (left innominate anterior rotation), ribs (right ribs 8–9 inhalation restriction).”
2. Note any related medical diagnosis
- Clinical Reasoning: Explain how the somatic dysfunction relates to the patient’s symptoms.
- Severity / Priority: Rate severity (if using a scale) or rank priorities for treatment. -
Plan: This covers what you will do, including OMT, other treatments, patient instructions, follow-up.
Sections to include:
- OMT Treatment Plan:
1. Regions treated: Which somatic dysfunction regions will you treat (or did treat).
2. Techniques used: Specify exactly which OMT techniques (using standard osteopathic terminology). The American Academy of Osteopathy guides list common abbreviations: e.g., ME (Muscle Energy), HVLA (High-Velocity Low-Amplitude), MFR (Myofascial Release), CS (Counterstrain), BLT (Balanced Ligamentous Tension), etc.
3. Treatment dosage / units: If billing, note how many body regions were treated, which helps decide CPT / billing codes. According to AAO forms, there are categories (e.g., 5–6 areas, 7–8 areas, 9–10 areas) for OMT billing.
4. Patient response: Immediately after treatment, what changed? Use ‘response’ boxes or narrative: e.g., “After ME, range of motion improved in lumbar flexion, tenderness reduced from 6/10 to 3/10, patient reports subjective loosening.”
- Adjunctive Therapies / Other Treatments:
1. Exercises: Prescribe specific exercises (home stretching, strengthening).
2. Lifestyle advice: Ergonomics, posture, sleep, hydration, stress reduction.
3. Referrals: Physical therapy, imaging, lab tests if needed.
- Follow-up Plan:
1. Review: When to return for the next OMT or review.
2. Monitoring: What to watch for (symptom changes, side-effects).
3. Patient homework: Self-care, exercises, posture modifications.
- Billing / Coding Notes (if relevant):
1. E/M code + OMT procedure code, if performed in the same visit. According to billing guidance, you need to support the somatic dysfunction regions and the treatment performed.
2. Also note documentation of consent, risk/benefit discussion if needed.
The Conclusion
Customized specialty templates are no longer “nice to have”—they are now an essential part of smooth clinical practice. With RevMaxx, healthcare providers get templates that match the way they work, reduce the time spent on paperwork, and support accurate documentation for every visit. Whether it’s cardiology, pediatrics, orthopedics, mental health, or any other specialty, RevMaxx builds templates that fit real workflows and real clinical needs.
By offering structured sections, smart prompts, and clean layouts, RevMaxx helps clinicians stay focused on patient care instead of typing notes for hours. The goal is simple: less effort, fewer errors, and more clarity in every chart.
RevMaxx brings efficiency, accuracy, and ease to everyday documentation—so providers can spend more time doing what truly matters: caring for their patients.